“Poisonous Venom May Be Just What Doctor Ordered”, Says Octogenarian
By Tom Wells, THE ASSOCIATED PRESS
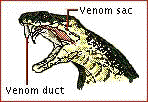
PUNTA GORDA, Fla. — Bill Haast slid back the top to the large metal box and up popped a cobra.
The snake spread its hood, weaved back and forth, side to side, then hissed. Haast placed his hand about six inches from its menacing fangs. A few drops of the snake’s venom could kill an ordinary human. Or, Haast believes, perhaps save someone. Bill Haast is not an ordinary human.
The snake lunged four times. Each time, Haast pulled back his hand, just out of range, just in time.
His timing has not always been perfect. At 85, he has been bitten 162 times — the latest, by a cobra, three months ago — by snakes with venom poisonous enough to kill an elephant. Twice, Haast almost died. But Haast has been injecting himself with snake venom since 1948. He has built up such powerful antibodies in his system that his blood has been used as a snakebite antidote. He began with tiny amounts of rattlesnake venom and built up the dosage over the years. He injects himself once a week with venom from 32 species. He says he is now immune from snakebites.
He also believes the snake venom has kept him healthy and holds the potential to help people with multiple sclerosis and other diseases. Except for rare snakebites, he says, “I’ve never been sick a day in my life. I’ve never been to a doctor. I’ve never had the flu, not even a cold.” Neither, he says, has he had arthritis, bursitis or any communicable disease. He has never taken medicine, not even aspirin. He looks like a man in his 60s.
He walks with a spring in his step and his back ramrod straight. He spends hours each day at his serpentarium in southwest Florida pulling weeds and planting shrubs in a two-acre plot where he hopes to breed snakes. He puts his hands on the 4-foot wall and vaults over.
Is snake venom the secret to health and long life?
“Come back in 15 years when I’m 100, and if I still look like I do today, then I would say `yes,’ ” Haast says. He believes venom can be useful against arthritis and other diseases. He produced a drug in the late 1970s that a Miami doctor used at a clinic to treat multiple-sclerosis patients. But the Food and Drug Administration closed down the clinic.
The new serpentarium Haast is working on will be his second snake-raising operation in Florida. Just after World War II he opened a serpentarium and tourist attraction south of Miami and ran it for nearly 40 years. Then he lost heart. Already disappointed by the FDA’s rejection of what he saw as groundbreaking work in finding a medical use for snake venom, he became disturbed and distraught by the death of a child who fell into a crocodile pit and was attacked.
He sold out in 1984 and moved to Utah.
In Utah, Haast continued extracting venom for snakebite antitoxin and for research. He found he missed Florida’s climate and landscape and returned six years ago. His new serpentarium is along a crushed-rock road not far from Punta Gorda (Wide Spot, in Spanish) in rural southwestern Florida. He no longer does shows for tourists.
He has about 400 snakes, extracts their venom daily and sells it to laboratories. A gram of venom from an African tree snake goes for $6,000; sea snake venom $3,000; cottonmouth venom $60. “We don’t need to do this, but there is nothing else to do and I want to make sure researchers get what they need,” Haast says.
The garage behind the new home he and his wife Nancy are building shelters a red Cornice II Rolls-Royce convertible (hers) and a white 1956 Lincoln Continental (his) in showroom condition.
Haast was born in 1910 in Paterson, N.J., and caught his first snake when he was 7. When he was 12 a copperhead bite put him in the hospital. He had grabbed the snake by the tail and learned a lesson: wrong end. He came to South Florida in the late 1920s and worked with a man who had a traveling roadside snake show for tourists. The Depression dried up business, so he took to making moonshine out in the Everglades. That gave him an opportunity to catch snakes.
During World War II he had a chance to buy more exotic poisonous snakes when he flew with Pan Am
crews that delivered food and medicine to Africa and Asia.“While the rest of the crew was hitting the bars I would be buying snakes,” he recalls.
After the war, Haast was so consumed with his serpentarium project, he says, that it destroyed his first marriage. His son stayed with him to help clear the land. The two lived in a shack, ate from cans and bathed in barrels.
Haast opened the serpentarium in 1948, performing with snakes for tourists and selling venom from about 36,000 extractions annually. He was confident that cobra venom held the secret to curing or maybe even preventing disease. His built-up immunity to snake venom certainly saved his own life.
In 1954 he was bitten by a blue krait, a snake that comes from Asia. Drop for drop, the krait’s venom is
many times more poisonous than a cobra’s. “I had never heard of a krait bite victim ever surviving,” Haast says. “I felt like the skin had been stripped from my body, like every nerve in my teeth was exposed, like my hair was being ripped out of my head.” Haast survived, barely. The snake died 10 days later.
The remarkable thing about Haast’s encounter with the krait was that, despite his agony, he insisted on
making notes. He scribbled that he had a sore throat, sore jaw muscles, blurred vision, chest and stomach spasms. When, three hours after the bite, he could no longer write, he dictated, noting his belief that the venom could not affect every nerve in his body and not have some use in medicine.
Indeed, his own blood has such a use.
In 1969, he answered an emergency summons from Bob Elgin, director of the Des Moines Zoo in Iowa, who had been bitten by a snake. Blood transfusions from Haast saved him. Haast keeps a letter from Elgin: “Each morning when the sun comes up, I think of you.”
Haast’s chance to test his theory, however, resulted in his run-in with the FDA. An FDA document provides details: In the late 1970s, A Miami physician named Ben Sheppard (now dead), suffered from rheumatoid arthritis. Sheppard took PROven, the medication produced by Haast. The doctor was so pleased with the results that he started giving injections to patients with a variety of diseases.
Sheppard’s clinic became famous, and was featured on the CBS-TV show “60 Minutes.” Haast recalls:
“Sheppard eventually was treating six or seven thousand patients. Most of them had MS. People came from all over the United States and even from other countries. The drug really helped them, but the FDA was upset because we hadn’t done clinical studies first.” Just so. The FDA shut down the clinic and banned the drug. It ruled that the drug had not been properly tested or licensed for human use.
The Multiple Sclerosis Society still gets so many inquiries about PROven that it felt compelled to publish something on the drug last year. The article notes the drug has been suggested as a treatment for arthritis, lupus, herpes simplex, herpes zoster, muscular dystrophy, Parkinson’s disease, myasthenia gravis and amyotrophic lateral sclerosis.
Although PROven has been banned by the FDA, a similar mixture known as Horvi MS9 is sold legally in drugstores in Germany, the MS Society said.
Time will judge whether Haast was prophetic in his belief that snake venom can be beneficial to mankind. One of Haast’s favorite authors is Jules Verne, the 19th-century science-fiction writer ridiculed for his novels about men going to the moon and traveling in submarines.
Of his own theories, Haast says, “We’ll see.”
John Klein’s note: I have recently written a page with more info on the controversial treatment of MS with snake venom.